Lasik-PRK
4/23/2018 9:46:31 AM
View: 1669
How images are formed in the eye
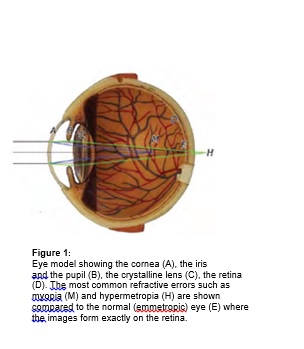
Rays of light enter the eye (Figure 1) through its front surface, which is called the cornea (A), go through the hole in the iris, which is called the pupil (B), and travel through the crystalline lens(C). The cornea and lens are responsible for focusing the rays onto the retina (D), the light sensitive layer at the back of the eye. The retina converts light rays into impulses and these ar sent to the brain via the optic nerve. At the brain level the impulses are recognized as images. Around 2/3 of the eye’s focusing power comes from the cornea and 1/3 from the lens.
Refractive errors
Myopia (nearsightedness):
In an eye with Myopia the corneal focusing power is too strong for the eye’s overall length. Images fall in front of the retina rather than being focused onto it and the vision is blurred (M).
Hypermetropia / Hyperopia (farsightedness):
In an eye with hypermetropia, the corneal focusing power is too weak for the eye’s overall length. Images fall behind the retina rather than being focused onto it and the vision can be blurred (H).
Astigmatism:
Astigmatism occurs when the cornea is more curved in one direction (a meridian) compared to
another. In these cases the cornea is shaped more like a rugby ball rather than a football. If astigmatism is significant, images reaching the retina are stretched and distorted and the vision is blurred.
High order aberrations (HoA):
Sometimes the visual problems are more complex than the ones described above. This typically occurs when the corneal surface is irregular. The most frequent high order aberrations are Spherical Aberration and Coma, but there are many more of them. HoA can be the result of previously complicated surgery, trauma or different eye conditions. In eyes with HoA the quality of the vision is typically poor even if glasses or soft contact lenses are worn and the only valuable option may be either wearing a hard or a gas permeable contact lens, or undergoing laser refractive surgery.
Refractive surgery
Most refractive errors can be corrected (or at least improved) by means of Refractive Surgery. This is a generic term, which comprises both Laser Refractive Surgery and correction by means of lens implants inside the eye. The latter is called Phakic intraocular lens (IOL) surgery.
Am I a good candidate for Refractive Surgery?
Not everyone is suitable for Refractive Surgery and your Corneal Specialist will advise you
whether you are or not. We have strict inclusion criteria to minimize complications and to ensure
a long lasting result. Minimum age normally is 21, you should not be pregnant or nursing, and
should be free of any corneal disease. The glasses or contact lens prescription should be stable for at least one year. You must be willing to accept the potential risks, complications and side effects possibly associated with each procedure
Laser refractive Surgery
General principles of laser refractive surgery: Laser refractive surgery involves using an Excimer laser (specialist ophthalmic laser) to reshape the cornea and permanently modify its refractive power (making it either weaker or stronger). The laser beams are targeted in a very precise way via a 6-D tracker which scans and follows the eye movements 500 times each second.principles To treat myopia, the surgeon uses the laser to remove a circle of central corneal tissue, thereby flattening the cornea and weakening the focusing power of the eye. The tissue is removed in a sophisticated way programmed into the computer by the surgeon. When myopia is very high or when the cornea is too thin, laser may not be safe anymore, as this would require too much tissue to be removed and the cornea could potentially become weak (there would be a risk of developing keratoconus). In these cases Phakic IOL surgery may be a possible alternative, provided that your eyes are suitable.
To treat hypermetropia, the surgeon uses the laser to remove a toroid (a doughnut shape) of
peripheral corneal tissue, thereby steepening the central cornea to increase the focusing power of the eye.
To treat astigmatism, the laser removes tissue in an elliptical pattern, selectively reshaping only some areas of the cornea in order to form a smooth and symmetrical surface (imagine
transforming a rugby ball into a round basketball).
To treat High Order Aberrations, a sophisticated Corneal or Ocular Wavefront Treatment is needed. This is a customized treatment based on your specific Corneal or Ocular Wavefront aberrations. Phakic IOLs cannot be used to correct HoA.
Types of Laser refractive surgery:
Laser refractive surgery can be divided into two broad categories: LASIK and SURFACE ABLATIONS. In LASIK a flap is lifted and the main laser reshaping is carried out under the flap whereas in SURFACE ABLATIONS the reshaping is done directly on the corneal
surface.
Surface ablations
In SURFACE ABLATIONS, the epithelium (the outermost layer of the cornea which regenerates
spontaneously every few days) is removed using different techniques (PRK, LASEK, Epi-LASIK, Trans-PRK). This is like creating a scratch on the eye surface, but in a controlled manner. Then the laser excimer (exactly the same laser used for LASIK) reshapes the stroma, the underlying layer.
A zero-power bandage contact lens is applied to protect the eye while the epithelium heals,which occurs in 4-6 days. Surface ablations are more uncomfortable initially than LASIK, but are ideal in patients with thin corneas and in those ones whose occupation or hobbies make it more dangerous to have a flap, as this could be dislodged accidentally (this applies to army personnel, professional fighters, extreme sportsmen).
The only aspect in which surface ablations differ from each other is the way in which the epithelium is removed. In PRK (PhotoRefractive Keratectomy) the epithelium is removed mechanically by the surgeon using a blunt instrument. In LASEK (LAser Sub-Epithelial Keratectomy) it is removed mechanically by the surgeon using a diluted alcohol solution and a blunt instrument (the alcohol makes it easier and less traumatic to remove the epithelium compared to PRK). In Epi- LASIK the epithelium is removed using a machine with a blunt blade while in TRANS-PRK instead the epithelium is entirely removed by the laser and the eye is hardly touched by the surgeon.This is the latest procedure but it is not suitable for all refractive errors. In SURFACE ABLATIONS the vision recovers Slowly, not allowing you to resume your work for at least 5-7 days. Typically the vision won’t be good enough to drive for around 1 week after surgery. The vision will not be very sharp for around 1 month after surgery, but most often it will be reasonably good already afte acouple of weeks. In some patients the vision may take longer to improve.
In SURFACE ABLATIONS the eyes are uncomfortable or painful and very sensitive
to light for around 3-5 days.
Typically patients need to come back for follow up visits after 1-2 days from surgery and then
after 1 and 3 months.
SURFACE ABLATIONS
No-flap, longer healing, more discomfort, ideal in thin corneas.
- PRK
- LASEK
- Epi-LASIK
- Trans PRK
Will I ever need to do it again?
Sometimes an enhancement (extra treatment) is needed if your vision is not fully corrected after the first 3-4 months or if it deteriorates later. The second situation is called regression and it can happen either months or years after the original procedure. In case of LASIK, enhancements can be done by simply lifting the original flap, whereas in Surface Ablations the original procedure needs to be repeated again and recovery is equally slow as after the first surgery. Sometimes eyes which underwent LASIK many months before may need to have new flaps created rather than the old ones lifted and occasionally it may be better to perform a Surface Ablation on top of an old LASIK flap, rather than lifting this up.
What are the risks, complications and side effects?
As with any operation, complications with LASIK and Surface Ablations are possible, but fortunately they are quite rare. Undercorrection or overcorrection or development of astigmatism can occur but can generally be improved with glasses, contact lenses, or by additional laser surgery. Most complications can be treated without losing any vision and permanent vision loss is very rare. It can happen that your vision will not be as good after surgery as before, even with glasses or contact lenses.
Almost everyone experiences some dryness and fluctuating vision during the day. For most people these symptoms fade within one month, although some people may continue to have symptoms for a longer period of time. Other side effects may include red patches on the sclera (the white part of the eye) for a few weeks after LASIK, discomfort, blurry vision, dryness, scratchiness, glare, halos or starbursts around lights and light sensitivity.
Most of these side effects disappear over time, but in rare situations they may be permanent. Infections are possible but they normally clear well with antibiotics. Even after refractive surgery, certain people may still need to wear glasses or contact lenses.
contact lenses and glasses each have their benefits and drawbacks. Neither LASIK nor Surface Ablation correct presbyopia, the age related loss of the close-up focusing power due to stiffness of the crystalline lens. With or without refractive surgery, almost everyone who has excellent distance vision will need reading glasses by the time they reach their early forties.
دیدگاه های ارسال شده توسط شما، پس از تایید مدیر سایت در وب سایت منتشر خواهد شد.
پیام هایی که حاوی تهمت یا افترا باشد منتشر نخواهد شد.
پیام هایی که به غیر از زبان فارسی یا غیر مرتبط با خبر باشد منتشر نخواهد شد.